
The Armor You Cannot See: Why Bone Density Is the Most Overlooked Performance Metric

Bone mineral density is not an aging metric. It is a performance metric. Learn how DEXA scans measure the structural armor that determines your long-term durability, and why your T-score matters more than you think.
There is a metric that governs your ability to run, lift, climb, and absorb impact for the next three decades. It predicts fracture risk better than pain levels, better than how you feel after a hard session, and better than any performance benchmark you've been tracking.
It is your bone mineral density.
Most people will go their entire lives without measuring it. They'll track their weight, monitor their heart rate, count their macros, and log their workouts — and never once inspect the structural frame that supports all of it. They'll learn about bone density the way most people do: when something breaks.
By then, the intervention window has narrowed considerably. The structural deficit that caused the fracture has typically been building for a decade or more. The question was never whether the bones were strong enough today. The question was whether anyone measured them before the failure point arrived.
This article is about that measurement — what it reveals, why it matters earlier than most people think, and how it connects to the broader framework of long-term physical durability.
What Bone Mineral Density Actually Measures
Bone mineral density (BMD) quantifies the mineral content — primarily calcium and phosphorus — per square centimeter of bone tissue. Higher mineral content means denser, stronger bone. Lower mineral content means bone that is more porous, more fragile, and more susceptible to fracture under forces that healthy bone absorbs without incident.
The clinical standard for measuring BMD is dual-energy X-ray absorptiometry — the DEXA scan. The same technology that measures body composition with precision also measures bone density at the two skeletal sites most predictive of fracture risk: the hip and the lumbar spine.
The output is your T-score — a comparison of your bone density to the peak bone mass of a healthy 30-year-old of the same sex. The World Health Organization classifies T-scores into three categories:
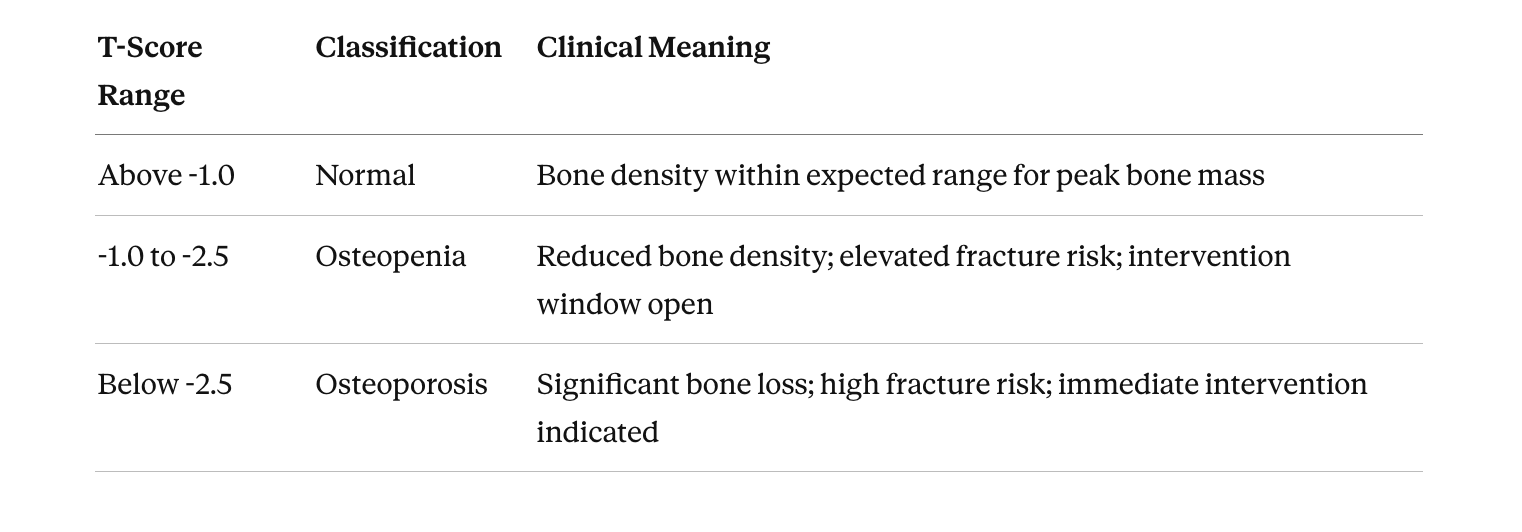
These categories are clinically useful, but they tell only part of the story. A T-score is a population comparison. It doesn't tell you how your bone density interacts with your lean mass, your training demands, or your cardiovascular output. It doesn't tell you whether the structural frame can support the performance you're asking of it.
That interaction — between skeletal integrity and the rest of the machine — is where the real insight lives.
Why Bone Density Matters Before Age 50
The conventional narrative positions bone density as a concern for post-menopausal women and elderly men. The clinical reality is different.
Peak bone mass is reached by approximately age 30. After that, density declines at a rate of 0.5–1% per year in both men and women. In women, that rate accelerates significantly during the five to seven years following menopause, when estrogen levels drop and bone resorption outpaces bone formation.
The decline begins decades before menopause. A 35-year-old woman who has never measured her bone density has no way of knowing whether she entered the decline phase with a strong structural foundation or a marginal one. A 40-year-old man who trains intensively has no way of knowing whether his skeletal system can sustain the loading demands he places on it every week.
The statistics are sobering. One in two women and one in four men over 50 will experience an osteoporotic fracture in their lifetime. Hip fractures in particular carry significant mortality risk — approximately 20% of hip fracture patients over 65 die within one year. The downstream effects on mobility, independence, and quality of life are well-documented.
The intervention window is before the fracture. The width of that window depends entirely on when the measurement happens.
The Training Connection: Loading, Impact, and Structural Adaptation
Bone is living tissue. It responds to mechanical stress through a process called mechanotransduction — the conversion of physical forces into biological signals that stimulate bone formation. When bone is loaded beyond its habitual threshold, osteoblasts (bone-building cells) are activated and mineral deposition increases.
Resistance training and impact exercise are the two most effective non-pharmacological interventions for maintaining and building bone density. Axial loading — exercises that compress the spine and hips under load, such as squats, deadlifts, and weighted carries — directly stimulates bone formation at the sites most vulnerable to fracture.
There is a critical nuance here: the loading must exceed the habitual threshold. Walking, while beneficial for many health outcomes, does not produce sufficient mechanical stress to stimulate meaningful bone adaptation in most adults. The stimulus must be progressive, site-specific, and sufficient in magnitude to trigger the remodeling response.
Without knowing your current bone density, you cannot calibrate the loading stimulus appropriately. Too little load and no adaptation occurs. Too much load on a compromised frame and stress fracture risk increases. The DEXA scan provides the baseline that makes the loading prescription precise rather than approximate.
The Nutritional Foundation
Mechanical loading provides the stimulus. Nutrition provides the raw materials.
Calcium and vitamin D are the most widely discussed nutrients for bone health, and for good reason. Calcium is the primary mineral component of bone tissue, and vitamin D is essential for calcium absorption. The nutritional picture extends beyond these two nutrients.
Protein intake — calibrated to lean mass rather than total body weight — supports the collagen matrix that gives bone its flexibility and resistance to fracture. Magnesium, vitamin K2, and zinc all play supporting roles in bone mineralization and remodeling.
Most nutritional recommendations for bone health are generic. "Take 1,000 mg of calcium daily" does not account for individual absorption rates, dietary intake, or the interaction between calcium supplementation and cardiovascular risk. A nutrition strategy built on actual DEXA data — knowing your current density, your lean mass, and your metabolic rate — produces a more targeted and effective approach.
Bone Density as a Cylinder: The Structural Engine
Within the Longevity Engine™ framework, bone density is a core component of the Structural cylinder — alongside lean mass and neuromuscular power output.
The Structural cylinder determines the integrity of the frame. It answers one fundamental question: can the physical structure support the demands being placed on it?
When the Structural cylinder is strong — dense bones, adequate lean mass, sufficient power output — the frame absorbs impact, sustains loading, and recovers from physical stress. When it is weak, the frame becomes the limiting factor regardless of how capable the other cylinders are.
A person with elite cardiovascular output and declining bone density is running a powerful engine on a thinning frame. The cardiovascular system can sustain the effort, but the skeletal system cannot absorb the repetitive impact. The constraint is structural, and no amount of cardiovascular training will address it. This is the core logic behind identifying the constraint before prescribing the intervention.
The Longevity Engine Read Tool includes bone density T-score as a direct input for this reason. It is one of the most consequential numbers in the entire assessment — and one of the least commonly known.
The Bottom Line
Bone mineral density affects every person who intends to remain physically capable for the long term. The measurement takes ten minutes. The output is a single number — your T-score — that tells you whether your structural armor is intact, thinning, or compromised. That number changes the loading prescription, the nutritional strategy, and the long-term trajectory of your physical durability.
If you know your T-score, enter it into the Longevity Engine Read Tool and see where your Structural cylinder stands. If you don't know it, that gap is exactly what the tool is designed to surface.
Try the Longevity Engine Read Tool
Book your DEXA scan at DexaFit Seattle/Renton
Frequently Asked Questions
What is bone mineral density and why does it matter?
Bone mineral density (BMD) measures the mineral content per square centimeter of bone tissue. It determines skeletal strength, fracture resistance, and the structural integrity of the frame that supports every physical activity you perform.
How is bone density measured?
The clinical standard is a DEXA scan (dual-energy X-ray absorptiometry), which measures BMD at the hip and lumbar spine — the two sites most predictive of fracture risk.
What is a T-score?
Your T-score compares your bone density to the peak bone mass of a healthy 30-year-old of the same sex. Above -1.0 is normal; -1.0 to -2.5 is osteopenia; below -2.5 is osteoporosis.
At what age should I start measuring bone density?
Peak bone mass is reached by approximately age 30, and density declines after that. A baseline DEXA scan in your 30s or 40s provides the reference point that makes future measurements meaningful.
Can exercise improve bone density?
Yes. Resistance training and impact exercise stimulate bone formation through mechanotransduction. The loading must exceed habitual thresholds and target the specific skeletal sites where density is declining.
What role does nutrition play in bone health?
Calcium, vitamin D, protein calibrated to lean mass, magnesium, vitamin K2, and zinc all support bone mineralization and remodeling. A nutrition strategy built on DEXA data is more targeted than generic supplementation.
Is bone density only a concern for older women?
No. While post-menopausal women experience accelerated bone loss, men also lose density with age. One in four men over 50 will experience an osteoporotic fracture.
How does bone density relate to the Longevity Engine™ framework?
Bone density is a component of the Structural cylinder, which determines whether the physical frame can support the demands placed on it by the other cylinders (Cardiovascular, Metabolic).
How often should I retest bone density?
For most adults, retesting every 1–2 years provides sufficient data to track trends. If you are in the osteopenia range or actively intervening, annual testing is recommended.
What is the Longevity Engine Read Tool?
It is an interactive assessment that scores your Cardiovascular, Structural, and Metabolic cylinders against age- and sex-specific reference ranges, identifies your primary constraint, and assigns an Engine Status. Try the Longevity Engine Read Tool